

How Much Money Is Given To Illegal Immigrants In Health Care
Summary
In 2020, there were 22.1 one thousand thousand noncitizens in the United states of america, accounting for well-nigh seven% of the total U.S. population. Noncitizens include lawfully present and undocumented immigrants. Many individuals live in mixed clearing status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens. One in four children has an immigrant parent, and the majority of these children are citizens.
Noncitizens are significantly more than likely than citizens to be uninsured. In 2020, among the nonelderly population, 26% of lawfully present immigrants and about four in ten (42%) undocumented immigrants were uninsured compared to less than one in ten (eight%) citizens. Amid citizen children, those with at least i noncitizen parent were significantly more likely to be uninsured every bit those with citizen parents (10% vs. iv%).
Research suggests that the changes to immigration policy enacted during the Trump administration contributed to increased fears among immigrant families virtually participating in programs and seeking services, including health coverage and care. These included policies focused on curbing immigration, enhancing immigration enforcement, and limiting the apply of public assist among immigrant families. The Biden administration reversed many of these changes and recently proposed a new rule that excludes non-cash benefits such as Medicaid and the Children's Health Insurance Program (Flake) from public accuse determinations. Even so, ongoing efforts will likely be needed to reduce fears and rebuild trust amid immigrant families.
The pandemic likely contributed to increased wellness and financial needs and declines in health coverage among immigrant families. Immigrants' work, living, and transportation situations put them at increased risk for potential exposure to coronavirus. Noncitizen immigrants besides faced risk of fiscal difficulties due to the pandemic, as many work in service industries, such as restaurants and food services, that suffered cutbacks during the early phases of the pandemic. At the aforementioned time, immigrants have had more limited access to COVID relief, and data suggest that immigration-related fears may have contributed to reluctance accessing COVID-nineteen vaccines.
Recent federal and state activity has focused on expanding access to health coverage for immigrants, but broad sustained efforts to rebuild trust and reduce fears also will exist of import for supporting the health and well-being of immigrant families. At the federal level, legislation has been proposed that would expand eligibility for wellness coverage for immigrants, though it faces no clear path to passage in Congress. In improver, states are standing to have up federal options to expand Medicaid and CHIP coverage for lawfully present immigrant children and pregnant people. Moreover, several states accept recently proposed or taken activity to aggrandize country-funded coverage to low-income people regardless of immigration status. Other recent activity may help increase enrollment amid immigrants who are eligible for coverage options. As noted, the Biden Assistants proposed new public charge rules, which may help reduce fears among immigrant families almost participating in non-greenbacks assistance programs, including health coverage. Further, the Administration increased funding for Navigator programs, which provide enrollment assistance to individuals. However, even with these deportment, it will likely accept time and sustained community-led efforts to rebuild trust and reduce fears surrounding the use of services amidst immigrant families.
Overview of Immigrants
In 2020, at that place were 22.ane 1000000 noncitizens and 22.vii million naturalized citizens residing in the U.Southward., who each deemed for about vii% of the total population (Figure one). Most 6 in 10 noncitizens were lawfully nowadays immigrants, while the remaining iv in ten were undocumented immigrants (meet Text Box one).one Many individuals live in mixed immigration status families that may include lawfully present immigrants, undocumented immigrants, and/or citizens.
A total of 19.2 million or one in 4 children had an immigrant parent equally of 2020, and the majority of these children were citizens. Nigh 9.7 million or xiii% were denizen children with a noncitizen parent.
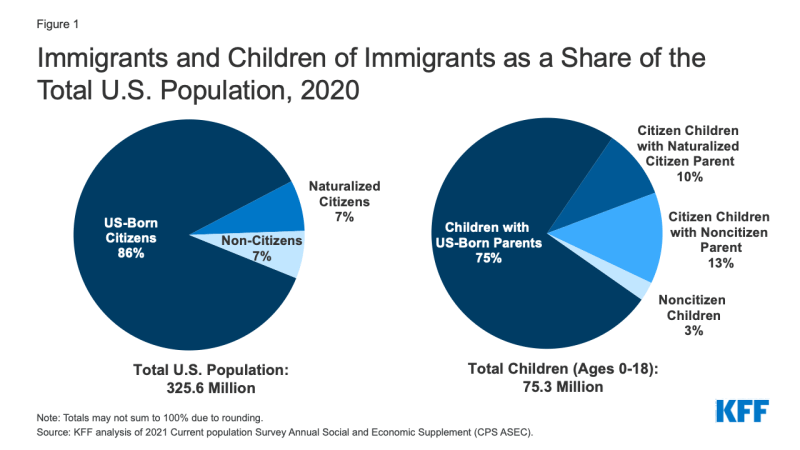
Effigy 1: Immigrants and Children of Immigrants every bit a Share of the Total U.S. Population, 2020
Text Box 1: Overview of Lawfully Present and Undocumented Immigrants
Lawfully present immigrants are noncitizens who are lawfully residing in the U.S. This group includes legal permanent residents (LPRs, i.e., "green card" holders), refugees, asylees, and other individuals who are authorized to live in the U.S. temporarily or permanently. Individuals who have received deferred action are authorized to exist nowadays in the U.S. and therefore considered to be lawfully present. Notwithstanding, individuals with Deferred Action for Childhood Arrivals status are not considered to take an clearing status that is eligible for federally-funded health insurance (come across below).
Undocumented immigrants are foreign-born individuals residing in the U.S. without say-so. This grouping includes individuals who entered the land without authorization and individuals who entered the country lawfully and stayed after their visa or status expired.
Health Coverage for Nonelderly Noncitizens
In 2020, more than than three-quarters (76%) of the 27.3 million nonelderly uninsured were U.S.-born and naturalized citizens (Figure ii). The remaining 24% were noncitizens.
However, noncitizens, including lawfully nowadays and undocumented immigrants, were significantly more than likely to be uninsured than citizens. Amongst the nonelderly population, 26% of lawfully nowadays immigrants and approximately iv in ten (42%) undocumented immigrants were uninsured compared to 8% of citizens (Figure 3).
These differences in coverage likewise occur amidst children, with noncitizen children more likely to lack coverage compared to their citizen counterparts. Moreover, amongst citizen children, those with at least one noncitizen parent were significantly more likely to exist uninsured every bit those with citizen parents (Figure 4).
Barriers to Health Coverage for Noncitizens
The college uninsured rate among noncitizens reflects limited access to employer-sponsored coverage; eligibility restrictions for Medicaid, Scrap, and ACA Marketplace coverage; and barriers to enrollment amid eligible individuals.
Although almost nonelderly noncitizens live in a family with a total-fourth dimension worker, they confront gaps in access to individual coverage. Nonelderly noncitizens are equally likely as nonelderly citizens to be living in a family with at least one total-time worker, but they are more probable to exist depression-income (Figure v). They take lower incomes because they are oft employed in low-wage jobs and industries that are less probable to offer employer-sponsored coverage. Given their lower incomes, noncitizens also face increased challenges affording employer-sponsored coverage when information technology is available or through the individual market.
Lawfully present immigrants may authorize for Medicaid and CHIP only are subject to sure eligibility restrictions. In general, lawfully present immigrants must have a "qualified" clearing status to be eligible for Medicaid or CHIP, and many, including most lawful permanent residents or "green card" holders, must await five years after obtaining qualified status before they may enroll. Some immigrants with qualified condition, such as refugees and asylees, do not accept to wait 5 years earlier enrolling. Some immigrants, such as those with temporary protected status, are lawfully present but exercise not take a qualified status and are non eligible to enroll in Medicaid or Flake regardless of their length of time in the land (Appendix A). For children and pregnant people, states can eliminate the v-year await and extend coverage to lawfully present immigrants without a qualified status. As of January 2022, 35 states have taken up this selection for children and half have elected the pick for pregnant individuals.
Lawfully present immigrants tin can purchase coverage through the ACA Marketplaces and may receive subsidies for this coverage. These subsidies are bachelor to people with incomes from 100% to 400% FPL who are non eligible for other coverage. In addition, lawfully present immigrants with incomes below 100% FPL may receive subsidies if they are ineligible for Medicaid based on immigration status. This grouping includes lawfully nowadays immigrants who are not eligible for Medicaid or CHIP because they are in the five-twelvemonth waiting period or do not have a "qualified" condition.
Undocumented immigrants are not eligible to enroll in Medicaid or Scrap or to buy coverage through the ACA Marketplaces. Under rules issued by the Centers for Medicare and Medicaid Services, individuals with Deferred Action for Babyhood Arrivals (DACA) condition are non considered lawfully present and remain ineligible for coverage options. Medicaid payments for emergency services may be made on behalf of individuals who are otherwise eligible for Medicaid but for their immigration condition. These payments encompass costs for emergency care for lawfully present immigrants who remain ineligible for Medicaid as well as undocumented immigrants. Since 2002, states have had the option to provide prenatal care to people regardless of clearing status by extending CHIP coverage to the unborn child. Equally of January 2022, xviii states have adopted this option. Unlike other pregnancy-related coverage in Medicaid and Scrap, which requires lx days of postpartum coverage, the unborn child option does non include this coverage. However, several states provide postpartum coverage, regardless of immigration status, either through a CHIP land plan amendment or using country-but funding. In improver, some states take state-funded health programs that provide coverage to some groups of immigrants regardless of immigration status. In that location are also some locally-funded programs that provide coverage or assistance without regard to immigration status.
Many uninsured lawfully present immigrants are eligible for coverage options under the ACA only remain uninsured, while uninsured undocumented immigrants are ineligible for coverage options. Prior to the pandemic many uninsured lawfully present immigrants were eligible for ACA coverage. The American Rescue Plan Act (ARPA) enacted in 2021 further increased access to health coverage through temporary increases and expansions in eligibility for subsidies to buy health insurance through the wellness insurance marketplaces. Information technology also includes incentives to states that have not yet adopted the ACA Medicaid expansion to do so and provides a new pick for states to extend the length of Medicaid coverage for postpartum women. With the temporary changes under ARPA, approximately three-quarters (77%) of uninsured lawfully present immigrants were eligible for coverage, including 31% who were eligible for Medicaid and 46% who were eligible for ACA subsidies (Figure 6). Uninsured undocumented immigrants are ineligible for coverage options due to their immigration status. In the absence of coverage, they remain reliant on prophylactic internet clinics and hospitals for care and frequently go without needed care.
Many lawfully present immigrants who are eligible for coverage remain uninsured because immigrant families face a range of enrollment barriers, including fearfulness, confusion about eligibility policies, difficulty navigating the enrollment procedure, and linguistic communication and literacy challenges. Research suggests that changes to clearing policy fabricated past the Trump administration contributed to growing fears among immigrant families about enrolling themselves and/or their children in Medicaid and CHIP even if they were eligible. In particular, changes to public charge policy that allowed federal officials to consider the utilize of sure not-cash programs, including Medicaid for not-pregnant adults, when determining whether to provide certain individuals a dark-green card or entry into the U.S., likely contributed to decreases in participation in Medicaid among immigrant families and their primarily U.S.-built-in children. The Biden administration reversed many of these changes, including the changes to public charge policy, and recently proposed new public charge regulations that exclude use of Medicaid and Chip, except for coverage of long-term institutionalized care, from public accuse determinations.
The pandemic likely contributed to increased health and fiscal needs and declines in wellness coverage among immigrant families. Immigrants' work, living, and transportation situations put them at increased adventure for potential exposure to coronavirus and its variants. Noncitizen immigrants also faced financial difficulties due to the pandemic, as many work in service industries, such as restaurants and food services, that suffered cutbacks. Initial job losses at the start of the pandemic were particularly loftier among immigrants, which likely contributed to increased financial stress and potential loss of health insurance, although many employment losses have rebounded since earlier in the pandemic. At the aforementioned time, immigrants faced limits on access to COVID-nineteen relief, and ongoing immigration-related fears made some reluctant to access assistance, services, and COVID-19 vaccines. Some states and localities, such equally California and New York, created programs to provide assistance to immigrants who were excluded from federal sources of COVID-19 assistance.
Proposals and Recent Deportment to Increase Access to Wellness Coverage for Immigrants
Contempo federal and state activity has focused on expanding admission to health coverage for immigrants. Moreover, other contempo activity may assistance increase enrollment among immigrants who are eligible for coverage options. Yet, across these deportment, broad sustained customs-led efforts volition probable be key for reducing fears and rebuilding trust among immigrant families.
In December 2020, Congress restored Medicaid eligibility for citizens of Meaty of Free Association (COFA) communities. Compacts of Free Clan are agreements between the U.S. authorities and the Republic of the Marshall islands, the Federated states of micronesia, and the Republic of Palau. Certain citizens of these nations can lawfully work, study, and reside in the U.S., merely they had been excluded from federally-funded Medicaid since 1996, under the Personal Responsibility and Work Opportunity Reconciliation Human action (PRWORA). As part of a COVID-relief package, Congress restored Medicaid eligibility for COFA citizens who come across other eligibility requirements for the program effective Dec 27, 2020.
Recent federal legislation has been proposed that would expand immigrant eligibility for health coverage, though there is no clear path to passage in Congress. In 2021, the Wellness Disinterestedness and Access Under the Law (HEAL) Act and Lifting Immigrant Families Through Benefits Access Restoration Human action (Elevator the BAR) Act were introduced into Congress. Both acts would remove the five-yr waiting period for wellness coverage and other assistance programs that currently employ to many lawfully present immigrants nether the 1996 PRORWA rules. They also would expand the definition of lawfully present immigrants to include Deferred Action for Childhood Arrivals (DACA) recipients and certain other immigrants who are authorized to be in the U.S., so that they could qualify for federally funded health care programs. In addition, the HEAL Act would permit undocumented immigrants to access health insurance coverage through the ACA Marketplaces and to be eligible for subsidies to kickoff the cost of this coverage. Both acts also would ensure that lawfully present immigrants with incomes below 100% FPL may receive subsidies if they are ineligible for Medicaid based on immigration status if they live in a state that has not expanded Medicaid.
Several states have proposed or taken action to expand coverage for immigrant children and meaning individuals. Currently, six states (California, DC, Illinois, New York, Oregon and Washington) provide comprehensive state-funded coverage to all income-eligible children, regardless of clearing status. Massachusetts provides primary and preventive services to all children, regardless of immigration status or income. Several states will extend Medicaid-like, state-funded coverage to immigrant children, including Maine and Vermont in July 2022, and Connecticut to children nether historic period nine in January 2023. New Jersey has also proposed to expand coverage to children currently ineligible due to clearing condition in the FY 2023 Governor'southward upkeep. A number of states also provide state-funded pregnancy coverage regardless of clearing status, including DC, New Jersey, and New York. DC plans to adopt the Scrap unborn child option in 2022 along with Connecticut and Maine, and Vermont will extend country-funded Medicaid-like coverage to pregnant individuals regardless of immigration status in July 2022. The American Rescue Plan Act gives states the option to extend Medicaid postpartum coverage from sixty days to 12 months offset in April 2022. V states—California, Connecticut, Massachusetts, Minnesota, and Washington—that are planning to take up this option volition also extend the coverage to postpartum individuals who are non eligible due to immigration status. California and Illinois recently implemented 12 months postpartum coverage regardless of clearing status through CHIP Wellness Services Initiatives amendments.
Some states are also taking action to expand fully state-funded coverage to adult immigrants. California Governor Gavin Newsom's 2022-2023 proposed budget would provide fully state-funded Medicaid coverage to all income-eligible adults, ages 26 to 49, regardless of clearing status, no sooner than January, i 2024. The land previously extended land-funded Medicaid coverage to immature adults ages 19-26 regardless of immigration status, and adults ages 50 and older will become eligible on May ane, 2022. In December 2020, Illinois extended land-funded coverage to low-income individuals ages 65 and older who were not eligible due to their immigration status. Equally of May 2022, coverage volition also be extended to low-income immigrants ages 55 to 64, regardless of immigration status, and proposed legislation would further aggrandize this coverage to all adults ages xix and older. In Oregon, the Cover All People Act, volition extend state-funded coverage to all low-income adults who are non eligible due to immigration status, starting on July 1, 2022, subject to available funding. Prior to this recent state activity, only the District of Columbia'due south locally-funded Healthcare Alliance program, created in 1999, provided health coverage to depression-income residents regardless of immigration status. States can too provide land-funded premium subsidies to immigrants who are ineligible for federal premium subsidies in the Marketplace due to their immigration status. In Colorado, beginning in 2023, state residents with income upwards to 300% FPL who do not authorize for wellness insurance under the Affordable Care Act or other public programs because of their immigration status volition be eligible for state-funded premium subsidies to assist them in purchasing private coverage.
The Biden Administration has proposed changes to public charge policies that are intended to reduce fears of enrolling in health coverage and accessing care. As noted, later taking part, the Biden administration reversed public charge policies implemented past the Trump Administration that had made some immigrant families more reluctant to admission health coverage and care for themselves and their children. More than recently, on February 24, 2022, the Assistants proposed new public charge regulations that would exclude use of Medicaid and Fleck, except for coverage of long-term institutionalized care, from public charge determinations. The proposed dominion would largely codify the 1999 field guidance that has been guiding public charge determinations since the Biden Administration reversed the 2019 Trump Administration changes to public charge policy. The rule would define a public charge as someone "probable at any time to become primarily dependent on the authorities for subsistence, as demonstrated by either the receipt of public greenbacks assistance for income maintenance or long-term institutionalization at government expense,". It likewise specifies factors that can be considered in public charge determinations and notes that public accuse determinations must exist made on the totality of circumstances. The proposed dominion volition be in a 60-day public comment period, until Apr 25, 2022, prior to it existence finalized.
The Administration has also increased funding for outreach and enrollment assistance, which may help eligible immigrant families enroll and stay enrolled in coverage. In Baronial 2021, CMS appear $eighty million in funding for lx Navigator programs in 30 states with Federally-Facilitated Marketplaces for the 2022 program year, significantly higher than the annual funding awarded in 2018-2020. Navigator programs must provide information that is culturally and linguistically appropriate and can assist individuals with renewing Medicaid coverage and help those who are no longer eligible for Medicaid transition to coverage through the marketplaces. This aid may be specially important for helping immigrant families enroll in and maintain coverage given the complex eligibility requirements for immigrants and potential linguistic barriers and fears of negative clearing consequences.
Looking Ahead
Although noncitizen immigrants are equally probable as citizens to work, they are significantly more likely to exist uninsured due to more express access to both public and private coverage. The pandemic has likely worsened the health and financial challenges faced by immigrants, every bit they take been at increased risk for exposure, have had more limited admission to assistance, and take more limited access to wellness care. Recent federal and land activeness has focused on expanding immigrant eligibility for health coverage. Moreover, the Biden Assistants's changes to public charge policy and increased funding for outreach and enrollment aid may assist increase access to health coverage for immigrant families. Still, even with increased eligibility and enhanced outreach and enrollment assist, information technology volition likely require time and sustained work, including community-led efforts, to rebuild trust and reduce fears among immigrant families about accessing health coverage and care.
| Appendix A: Lawfully Present immigrants by Qualified Condition | |
| Qualified Immigrant Categories | Other Lawfully Present Immigrants |
|
|
| SOURCE: "Coverage for lawfully nowadays immigrants," HealthCare.gov, https://world wide web.healthcare.gov/immigrants/lawfully-nowadays-immigrants/. | |
Source: https://www.kff.org/racial-equity-and-health-policy/fact-sheet/health-coverage-of-immigrants/
Posted by: martinbeemeart44.blogspot.com
0 Response to "How Much Money Is Given To Illegal Immigrants In Health Care"
Post a Comment